


Trans Health Data
That time I made Jesse Singal Upset

It will never not be funny to me when people try to dunk on me by saying that anyone can create an account on the internet and call themselves arbiter of something and that's why you shouldn't listen to me.
I find this hilarious because they are right. I am literally just some guy who made a gimmick account to entertain himself. I try to be thoughtful and thorough but I'll get plenty wrong. What's really funny, though, is when these are influential people who have outsized voices in their respective spheres of influence. Most recently it was Jesse Singal, who has 147k followers on twitter. Why are they are taking the time to bitch about some random gimmick account? I post memes dude, you are clearly punching down.
They do this because they know, deep in their hearts, that they aren't actually all that different from me. They are posters at their core, and they thrive when they get to post. Glad I could help! It ups my engagement.
Anyway this is a short post about Trans issues because that's why Jesse Singal was mad at me.
For background, it started because I retweeted Jesse's nemesis Michael Hobbes by saying that it's a data red flag that Jesse was saying data isn't collectible on Trans issues. He didn't like that I said he could advocate for better data collection and that I think he actually wants to reduce the number of Trans kids to 0.
Now I admit that I didn't read all of Mr. Singal's work before shitposting. See, he DOES say that we need to collect more data! Silly me. That's his entire thing in fact! He wants us to collect more data on Trans kids because we have so little. And why are we doing all these procedures on children when we don't have proper data?
Astute readers will note that saying "we shouldn't be doing interventions without proper study" is like saying "we should reduce Trans kids receiving care to 0" outside of studying it, but let's move on.
My issue with Singal and the rest of the Trans care skeptics is that they assign an extremely high bar to data acceptability and want to ignore anything we know currently because it doesn't exactly fit with what we want to try.
But in medicine this process is always way more loose than ideal. We try things, we study them, we see if they work. If they don't then theoretically we stop or ask why, and if they do we expand use and keep studying and keep asking why. Lots of things that show positive results early turn out to have been a bad idea. Lots of things we keep doing because it seems like it works but we aren’t totally sure why.
Which gets to transgender care. We have data on transgender care. Is it all good? No. It's mostly on adults but we have a growing amount of studies on children. It often uses survey data, which can be challenging. Some of it is out of date. But we do have it. And it's not all bad.
For example, regret rate studies1 show really low regret rates for people who undergo a medical transition. That's important to know! Jesse doesn't like this meta analysis, and yeah he's not wrong that it's insufficient, but it really isn't a bad study, and you can find similar numbers other places2 as well. Of course there are problems with relying on regret rate alone, but ignoring it seems way worse. Lots of people are saying they don't regret doing this. We should care about that.
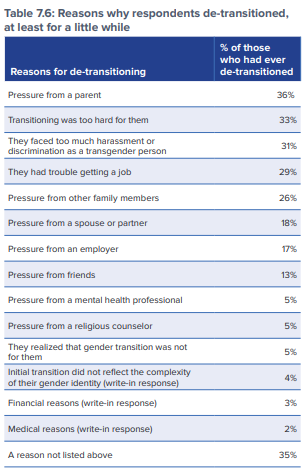
De-transition also seems to be more correlated with a lack of support network rather than personal reasons.
And Transgender children have high risk factors for other mental disorders, some of which may have a relationship to their gender dysphoria. Transgender youth also face discrimination and social stress3 that can cause downstream issues.
It’s not like hormone treatment has no side effects. There seems to be a correlation between hormones and a reduction in bone marrow density, but this could be because of when the drugs are given as the study says the same thing was not seen on children with precocious puberty (i.e. they receive the drugs at a much younger age). Plus, puberty blockers have shown positive effects as well.
While I’m not going to sit here and tell you that the science is settled, we are seeing a general consensus around what seems to be working. That is: We should be providing the Gender Affirming Care to children with Gender Dysphoria. To be clear, that isn’t saying everyone should immediately get reassignment surgery. Most of the care recommendations I’ve seen are to support social transitions of younger children and then do more intensive medical and surgical interventions after the child is sure this is who they are.
Data I’ve seen also does not support the claim that a mass number of children are getting medical interventions. Reuters reports that there were 42k gender dysphoria diagnoses in 2021 but only 4k kids on hormone therapy, 1.3k on puberty blockers, and 282 top surgeries. This shows a 70% YoY increase from 2020 to 2021 in dysphoria diagnosis but only a 26% increase in puberty blockers, 35% increase in hormone therapy and a 10% increase in top surgery. That’s a 31% increase taken together4

As you can see, despite there definitely being an increase in gender dysphoria diagnoses, the increase in intervention has been comparatively small. And to my knowledge the skeptical crowd has yet to produce any data that is contrary to this.
The problem, in the mind of the skeptic, is that we should not see any increase in the use of gender affirming care while we also have so little data on it. The problem is that we DO have data on the issue, even if it isn’t enough. If we probe what data gender skeptics are looking for their argument breaks down.
Jesse replied to me that one thing he wanted to see was Randomized Control Trials, but we don’t do RCTs because we’ve decided that withholding gender affirming care is child abuse. But how exactly does one do a Randomized control trial that is sufficiently blind on a puberty blocker or transition surgery? Yes we gave you this medicine that stops your puberty but you still got your period? I'm sorry we can't tell you if you are in the control group or not, do you still have dysphoria?
I’ll quote this study that discusses this issue at length:
Because [puberty blockers] are effective in delaying puberty it would soon become evident to participants, researchers and outcome assessors who was in the active treatment arm and who was not. This breakdown of blinding would mean that there would be potential bias in the outcome assessments, both in relation to biological and psychological outcomes. It would also mean that participants allocated to the non-treatment arm of the study would be likely to either withdraw from the study at a much higher rate than in the treatment arm introducing potential bias, and/or be more likely not to adhere to the trial but seek puberty delaying treatment outside of the trial thereby adding a confounder.
The study goes on to say that we know the drugs are effective at delaying puberty (which is what the RCT can best understand) and what we really need to know is how these drugs impact patients long term both physically and psychologically, which the RCT is less inclined to work for since there are many confounders to gender dysphoria such as seeking further care. And that’s before we talk about ethical issues!
I'll accept his point that we should see more longitudinal studies and more studies in general because it's important to have more data, but Jesse expressed doubt on ALL current and future studies, basically saying that they are so flawed that they don't add anything of value. What?
To keep track this means that:
• Studies that are in adults or another country can never apply to American children
• All our current studies on GAC for children add virtually nothing to our knowledge base
• All future studies will be lacking in the same way
They’ve landed themselves into a position where we know nothing and we can never know anything. So how exactly does this make it possible to study whether or not we should be doing this? When I say that people want to reduce Trans kids to 0 this is what I mean. They are entirely skeptical of the scientific and medical process and give no room for us to learn more. In practice then we can both never give the care and then never measure it.
Hilariously, one person said that we should study the issue but not experiment on children. That's kind of what study means bro.
Their real answer is =they want to be able to say they want to study it further while it never actually happens. Because to the gender skeptic the important KPI isn't the efficacy of Trans Healthcare, it's how many people receive it.
This article was very helpful for me in collating some studies. If you have any others let me know!
I didn’t want to include this part in the main post, but here is the Plastic Surgery Statistics Report, 2020, from the ASPS National Clearinghouse of Plastic Surgery. It’s just hard for me to understand why gender affirming procedures get all the attention when we are doing tons of plastic surgery on teenagers for procedures that are absolutely gender confirming. They are just cis-gender confirming.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8099405/ | This is an oft-used study to show that the regret rate of surgery is 1%. There are some issues with it, but it’s largely a good survey of what we know. Singal didn’t like this study and classified it as “adults in 20th c Sweeden” and used that to claim that it doesn’t apply to “21st c kids in America”. Firstly, don’t use a study to extrapolate more than what it says. Secondly, the study has data from all over western Europe and the USA and does seem to include some studies with minors. It’s out of date, obviously, but that’s not enough to just throw the whole thing out! It has relevance even if it’s not fully representative of the issue today.
https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf | Another place that was adult only and is out of date. But this stat is used quite a bit as well > in a survey of trans people 8% de-transitioned after transitioning and 62% of those people are now “living full time in a gender different than the gender they were thought to be at birth.” And the reason they de-transitioned are mostly a lack of support. Assume some selection bias with the fact that this is a survey of people who are trans, but other than that (and this survey being from 2015, a new one has been conducted but is not available at time of writing) this is a valid data-point.
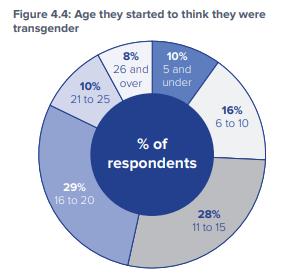
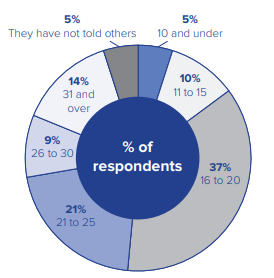
Another important point from this survey is age of transition. A full 54% of respondents said they started to think they were transgender before age 16 and 15% told others before they were 16. Part of the reason it’s been so hard to get good data on this is because so many kids don’t tell people so we can’t really study them all that well.
https://link.springer.com/epdf/10.1007/s10567-021-00344-6?sharing_token=pq6joxAQZg2iH4h2evdkhve4RwlQNchNByi7wbcMAY4zxQ4Mosl0jpyGMR6fS_ZKPdNc3AOWEEyvOyPpD8MIWm4cjxp0AFGnzDxlS328ZNYzKptc3usWCryNZEIb41v35udVZb5pDPF6KhtBmPuhwHnLbgpnq04TCqnU-fg3EkY%3D | This is a very good study that deserves much more attention that I’m going to give it. Again, there are some issues since this primarily uses survey data to learn things about trans kid’s lives. It also has only a limited focus on GAH and surgery, but that is by design. The main thing it showed is that having a good support network meant that people persisted with their trans identity and that having more isolation and less of a social network was associated with more problems.
Want to note here the statistical issues with adding together. It may be that the same child got more than one of these procedures either in the same year or the next year so this *may* slightly overstate the number of patients since I am not able to dedupe.
This is utterly pathetic.